 4.9 (400+
reviews)
4.9 (400+
reviews)

Introduction
Prescription refill calls take up more staff time than most practices realize. Between voicemails, portal messages, live calls, and after-hours requests, refill intake alone can consume hours of front-desk and nursing time every day.
For clinics handling hundreds or thousands of refill calls each month, this guide explains how to reduce that volume by up to 50% compromising clinical oversight or patient safety.
If you’re a practice manager, part of the front-desk team, a nurse, or a healthcare administrator looking to reduce refill-related workload without disrupting approval rules, keep reading!
AI Summary: Quick Steps to Reduce Prescription Refill Calls
Here’s how you can reduce prescription refill calls:
- Map and audit all current refill request channels
- Create a standardized refill intake process
- Collect required patient and medication details upfront
- Validate Information Before Staff Review
- Automate refill case creation inside the EHR
- Standardize refill intake logic across staff and systems
- Route only exceptions to nurses or providers
- Track volume, errors, and callback rates
What Is a Prescription Refill Workflow?
A prescription refill workflow is the process a healthcare practice follows from the moment a patient requests a medication refill to the moment the refill is approved, denied, or routed for review. It’s also where confusion around prescription refill vs prescription renewal often begins, leading to avoidable delays and staff follow-ups.
A typical refill workflow includes:
- Intake of the refill request
- Collection of patient identifiers
- Verification of medication details
- Eligibility check
- Routing to nurse or provider
- Communication back to the patient
When intake is unstructured or inconsistent, this workflow creates unnecessary rework, callbacks, and delays.

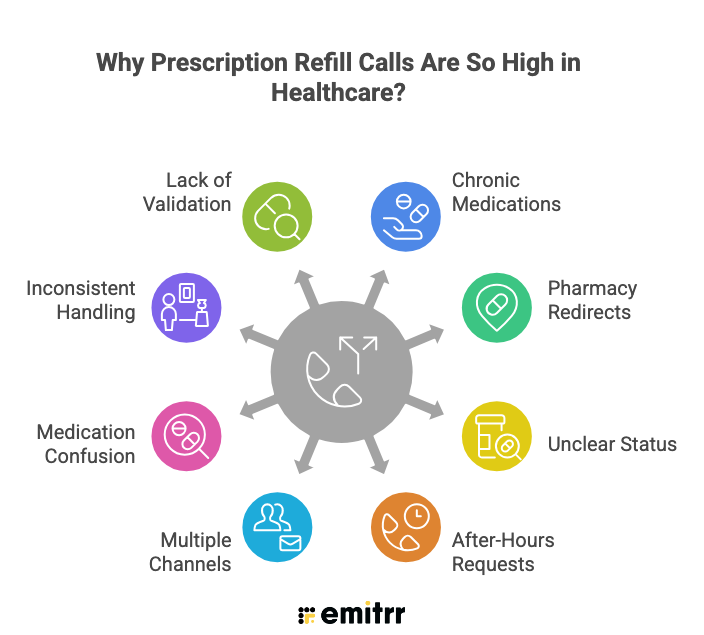
Why Prescription Refill Calls Are So High in Healthcare?
Medication refill calls remain one of the most persistent sources of inbound volume in healthcare. Patients keep calling about prescription refills, status approvals, pharmacy receipts, and unexpected delays. The pressure rarely comes from clinical complexity alone; it builds from recurring demand, fragmented intake, and communication gaps.
The following are the primary reasons refill call volume stays high.
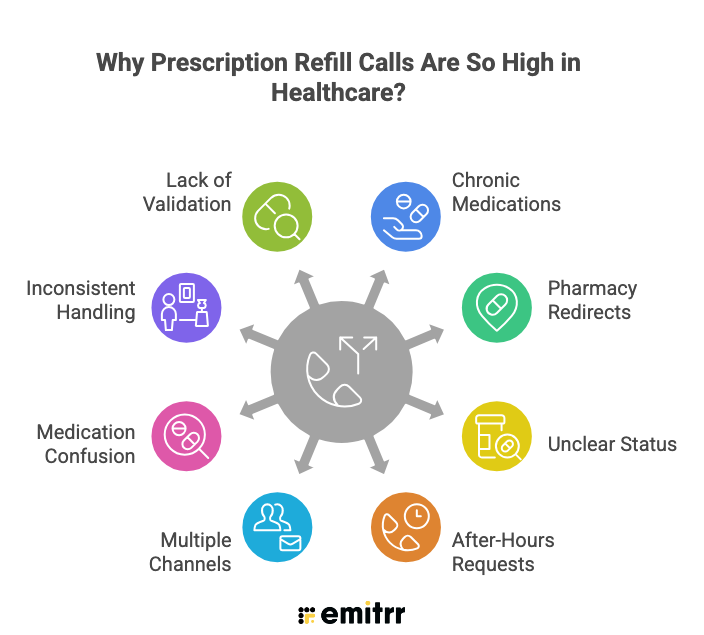
- Chronic Medications Create Recurring Demand
Refill demand never really stops. Many patients rely on long-term therapies for conditions such as hypertension, diabetes, asthma, and thyroid disorders. These prescriptions often run on 30-, 60-, or 90-day cycles.
The same patient may require refills multiple times each year. Even an efficient clinic experiences steady, predictable refill traffic. The core challenge is not the existence of refill calls; it is the way they enter and move through the system.
- Pharmacies Often Redirect Patients Back to the Practice
When refills are exhausted, prescriptions expire, or the original prescriber differs, pharmacies typically instruct patients to contact the doctor’s office.
From the patient’s perspective, they are following instructions. For the practice, this becomes another inbound call, even when the issue is procedural rather than clinical.
- Patients Are Unclear About Refill Status
A large portion of refill calls are status inquiries rather than new requests.
Patients frequently ask:
“Was my refill approved?”
“Did the pharmacy receive it?”
“Why was it denied?”
Absent a clear confirmation loop, patients assume an error occurred. The natural response is to call again, adding to the total volume.
- After-Hours Requests Accumulate Quickly
Refill requests do not occur only during business hours. Many patients think about medications in the evening when reviewing pill bottles or noticing a low supply.
When after-hours intake relies on voicemail, messages accumulate overnight. Staff begin the day managing a backlog instead of a clean queue. This increases perceived workload and response pressure. Customers report that around 1,300 refill calls per month were coming in, with a significant portion arriving after hours.
By morning, the staff is starting with accumulated requests rather than a fresh schedule. The backlog itself contributes to higher perceived call volume and operational strain.
- Multiple Intake Channels Multiply the Work
In many practices, refill requests come through live calls, voicemails, Athenahealth Patient Portal messages, and sometimes text messages. Each channel requires someone to manually interpret and enter the information.
Someone has to listen to the voicemail and then type it into the system. A nurse has to read the message in the patient portal and convert it into a refill request.
Even though these are “digital” channels, they still generate manual work. Volume feels higher because every request passes through multiple human steps.
- Medication Confusion Creates Follow-Up Calls
Another major driver of refill calls is medication confusion. Patients sometimes mispronounce medication names. They request medications that were discontinued. They ask for prescriptions written by another provider. In some cases, they do not even leave a clear name or date of birth in a voicemail.
When that happens, staff must call back to clarify. What started as one refill request becomes two or three calls. The total call count increases, even though the underlying need was simple.
- Inconsistent Front-Desk Handling Adds Hidden Volume
Your call notes also revealed that refill handling depends heavily on staff training. Some front-desk team members create structured refill requests. Others create generic cases. In some situations, staff are told to “just create everything as a case.”
When refills are not entered the first time correctly, nurses must rework them. They may have to re-enter medication details or convert cases into proper refill requests.
This internal rework does not always show up as an external call, but it increases processing time and slows response, which can trigger more patient follow-up calls.
- Lack of Real-Time Validation Increases Caution
Refill volume often feels high because practices cannot process requests quickly without proper validation.
When systems cannot confirm whether a medication is active, discontinued, or prescribed by the same provider, staff must proceed cautiously. This extends turnaround time. As response times increase, patients are more likely to call for updates. And, without structured intake and validation, each refill request carries uncertainty, and uncertainty leads to additional calls.
Although refill demand is naturally high in healthcare, the real operational strain does not come from request volume alone. It stems from how requests are received, interpreted, and processed once they reach the practice.
There’s a smarter way to reduce refill call volume by up to 40% and regain control of staff time. Watch how practices are using AI-driven refill automation to eliminate backlogs, minimize callbacks, and accelerate approvals across the entire workflow:
Understanding Why Prescription Refill Calls Overwhelm Practices
Prescription refill calls rarely overwhelm a practice because of volume alone. The strain typically builds from fragmented intake, missing information, and repeated manual handling.
Below are some key factors that explain where the pressure originates:
Refill Requests Come Through Too Many Channels
Refill requests enter through multiple paths, such as live calls, voicemails, patient portal messages, and SMS. Each channel presents information differently, with no consistent structure.
Staff must first interpret the request before processing it. Voicemails require listening, attempts to convert voicemail to text. Portal messages require reading and reformatting. Very few requests arrive ready for clinical review. Time is spent reconstructing details instead of evaluating the refill itself.
Voicemails Often Contain Incomplete or Unusable Information
Voicemail messages frequently lack critical identifiers or clear medication details. Patients may omit their date of birth, provide unclear drug names, or leave truncated recordings.
These gaps force staff to initiate follow-up calls. What should have been a single interaction expands into multiple touchpoints. Workload increases even though the underlying request remains simple.
Inconsistent Front-Desk Handling Creates Downstream Work
Refill intake quality often varies depending on staff training and workflow discipline, a challenge that becomes more visible in high-call volume environments. Some team members submit structured refill requests, while others create generic cases.
When requests are entered incorrectly, nurses must review, correct, or re-enter information. This downstream cleanup consumes clinical time and delays refill processing. The issue is not staff performance; it is workflow inconsistency.
Nurses Spend Time Re-Entering and Converting Requests
Instead of focusing purely on clinical decisions, nurses often manage administrative corrections.
They may need to:
- Confirm the correct medication
- Verify whether it was prescribed by the practice
- Check if it was discontinued
- Determine whether the request qualifies for refill or needs provider review
These steps are necessary but preventable when intake is structured from the start.
Medication Name Errors and Discontinued Prescriptions
Medication-related confusion adds significant friction. Patients may mispronounce drug names, request medications prescribed elsewhere, or ask for therapies no longer active.
Each ambiguous request requires manual investigation. Staff must cross-check charts, medication lists, and provider history before proceeding. Processing time expands, and queues grow.
Lack of Real-Time Validation Against the EHR
Many intake systems cannot:
- Validate medication against the active medication list
- Detect discontinued medications
- Confirm prescribing provider
- Distinguish refill vs nurse review in real time
This increases risk and slows throughput.
If your practice uses Athenahealth for prescription refills, see how AI-driven intake and workflow automation can dramatically reduce staff workload. Learn how practices save 70+ front-desk hours per month with no EHR replacement and no additional hiring:
High Monthly Refill Volume and After-Hours Burden
For high-volume practices, refill-related calls can exceed 1,000 per month. A large portion often arrives after hours, creating overnight accumulation.
Even modest reductions in intake errors or manual handling can produce meaningful workload relief. Improvements at the intake stage directly reduce nurse intervention, callbacks, and processing delays.
Summary Of Common Refill Intake Problems And Their Impact:
Prescription refill calls often feel overwhelming because small intake issues repeat across hundreds of patient interactions. Take a quick glance at where breakdowns occur and how they affect daily operations:
| Problem Area | What Happens | Operational Impact |
| Multiple intake channels | Requests come via calls, voicemails, portal messages, SMS | Staff must manually check and re-enter data from multiple systems |
| Incomplete voicemail messages | Missing DOB, unclear medication names, cut-off calls | Callback loops increase total call volume |
| Inconsistent front-desk handling | Some create refill requests, others create generic cases | Nurses must convert cases manually |
| Medication name errors | Mispronounced or incorrect medication names | Additional verification time required |
| No EHR validation at intake | Cannot detect discontinued or external prescriptions | Increased review risk and delays |
| High after-hours volume | Requests pile up overnight | Morning backlog for staff |
Prerequisites Before Reducing or Automating Refill Calls
Before introducing automation into refill workflows, confirm that a few foundational elements are clearly defined. This readiness checklist helps prevent safety gaps, routing errors, and processing delays:
✔ Establish which medications qualify for automatic renewal, which require nurse review, and which must go directly to a provider. Clear rules prevent unsafe automation.
✔ Specify who handles what. Structured routing avoids confusion, duplicate work, and misdirected requests.
✔ Accurate medication data supports proper validation, reduces false approvals, and prevents unnecessary investigations.
✔ Define how edge cases are managed, such as early refill requests, controlled substances, discontinued medications, or external prescriptions.
✔ Outline how refill requests submitted outside business hours are triaged, queued, and processed, and how prescription refill reminders guide patients to submit requests on time, preventing morning backlogs.
Manual Refill Workflow vs Structured Refill Intake Workflow
The difference between manual and structured refill intake is not subtle. It directly affects staff workload, error rates, turnaround time, and patient experience. The comparison below highlights where inefficiencies accumulate and where structured workflows create measurable relief:
| Aspect | Manual Refill Intake | Structured Refill Intake |
| Information capture | Staff listens to voicemails or read free-text messages | System collects required fields through guided prompts |
| Data quality | Often incomplete or unclear | Standardized, complete, and consistent |
| Staff effort | High manual interpretation and re-entry | Minimal correction or reconstruction |
| Callback frequency | High due to missing details | Reduced when data is captured correctly the first time |
| Error sources | Intake ambiguity and transcription mistakes | Significantly lower due to validation rules |
| Processing speed | Slower; requests require clarification | Faster; requests arrive ready for review |
| Nursing workload | Increased rework and case conversion | Focus shifts to clinical evaluation |
| Patient experience | Delays, uncertainty, repeat calls | Predictable updates and quicker resolution |
Step-by-Step Guide to Reducing Prescription Refill Calls
Follow this step-by-step guide to reduce prescription refill calls in your clinic:
Step 1: Map And Audit All Current Refill Request Channels
List every channel where refill requests arrive. Track monthly volume per channel. Identify which channels create the most rework.
Step 2: Create A Standardized Refill Intake Process
Choose a standardized intake method. This could be a structured phone flow, portal form, or AI-assisted intake tool.
The goal is to eliminate scattered and inconsistent requests.
Step 3: Collect Required Patient And Medication Details Upfront
Require:
- Full patient name
- Date of birth
- Medication name
- Dosage and frequency
- Preferred pharmacy
If information is incomplete, the system should prompt for clarification before submission.
Step 4: Validate Information Before Staff Review
Compare the requested medication against the active medication list. Flag mismatches, discontinued medications, or external prescriptions for manual review.
Step 5: Automate Refill Case Creation Inside The Ehr
Once intake is complete:
- Create a refill case automatically
- Attach all captured details
- Save conversation transcripts or recordings if applicable
This removes manual data entry from staff.
Step 6: Standardize Refill Intake Logic Across Staff and Systems
Use one intake logic every time. Questions and routing rules should not depend on staff experience or training level. Consistency reduces downstream confusion.
Step 7: Route Only Exceptions to Nurses or Providers
Not every refill requires deep review.
Use defined rules to determine:
- Which requests can move forward
- Which must be flagged
Staff should review structured cases and not decode messy voicemails.
Step 8: Track Volume, Errors, and Callback Rates
Monitor:
- Monthly refill volume
- Callback frequency
- Time spent per refill case
- Exception rate
Adjust intake logic based on patterns.
When You Should Not Fully Automate Refill Intake
Automation plays a powerful role in reducing routine refill workload, but not every scenario is appropriate for fully automated handling. Certain requests, including an emergency prescription refill, carry regulatory, safety, or clinical complexity that requires human evaluation. The situations below highlight where automation should support, not replace, clinical oversight:
Controlled Substances
Refills for controlled medications come with strict legal and safety requirements. These requests should always be reviewed and approved by a provider, even if intake is automated.
Complex Medication Changes
If a patient wants a dose change, reports side effects, or requests a different medication, it’s no longer a simple refill. These cases require clinical judgment and should be routed to staff.
Patients with Compliance or Safety Flags
Patients with a history of misuse, missed appointments, or documented safety concerns often require closer monitoring. A HIPAA-compliant AI agent can collect and document the refill request, but approval should remain under clinical supervision rather than a fully hands-off process.
Clinics Without Clean Medication Records
If medication lists are outdated or documentation is inconsistent, automation can create errors. Practices should clean up records before fully automating refill workflows.
How AI Agents Like Emitrr Support Structured Refill Intake
Emitrr offers an AI-powered patient communication layer that brings structure, speed, and consistency to refill intake and routine interactions. AI agents are transforming the healthcare industry by handling high-frequency requests such as prescription refills, appointment scheduling, and status inquiries through voice and SMS. Instead of staff decoding voicemails or re-entering fragmented messages, Emitrr’s AI agent captures complete information upfront, validates key details, and routes requests appropriately. As practices move to automate online medication refill with AI agents in 2026, Emitrr enables a safer, more efficient transition.
Here’s how AI agents like Emitrr simplify and support prescription refill intake, helping healthcare clinics reduce 50% call volume:
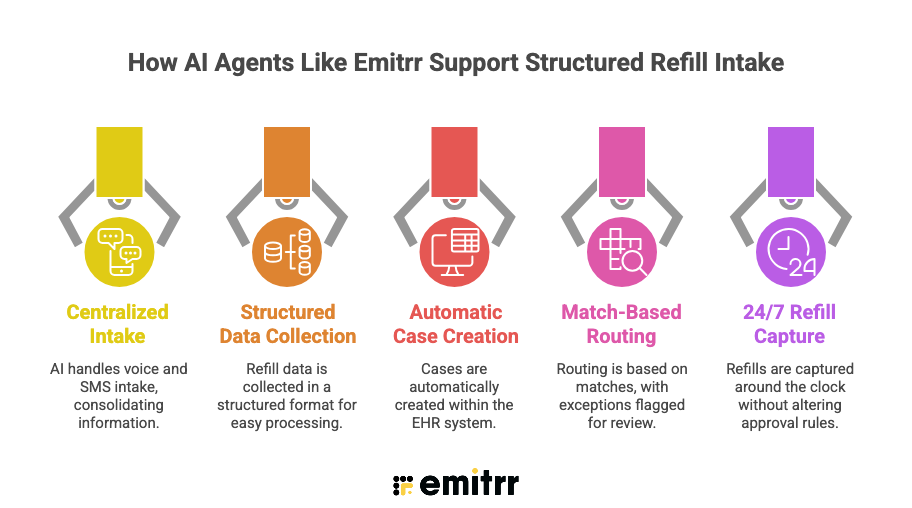
Centralized AI Intake for Voice and SMS
AI agents like Emitrr can act as the first point of contact for refill requests through both phone calls and text messages. This is where SMS-based prescription refill requests reduce call volume in healthcare by shifting routine refill interactions away from congested phone lines. Instead of patients leaving voicemails or speaking to different staff members, the AI handles the initial intake in one consistent way. Every request is captured in the same structured format, reducing confusion and repeat calls.
Watch Emitrr’s all-in-one AI agent in action. See how it automates calls, manages refill requests, and streamlines patient communication 24/7:
Structured Refill Data Collection
The Emitrr AI asks patients simple, required questions such as their name, date of birth, medication name, dosage, and pharmacy details. If something is unclear or incomplete, it asks again to make sure the information is correct. Each interaction creates a transcript and summary, so staff can quickly review what the patient shared without calling them back.
Automatic Case Creation Inside the EHR
Once all required details are collected, the system automatically creates a case inside the EHR with the patient’s information attached. Staff can begin reviewing the request immediately without retyping notes or listening to voicemails. This approach helps practices automate prescription refill requests without replacing your EHR. The existing approval process stays intact, but manual intake work is removed.
Match-Based Routing and Exception Flagging
If the refill request matches clinic rules, it moves forward for normal review. If something does not match, such as missing details or a flagged medication, it is clearly marked for closer attention. The AI does not approve medications; it simply ensures requests are complete and properly routed.
24/7 Refill Capture Without Changing Approval Rules
AI intake can capture refill requests even after clinic hours, preventing voicemail backlogs the next morning. Requests are organized and ready for review when staff return. Clinical decisions remain fully with the healthcare team.
Common Mistakes That Prevent Refill Call Reduction
Many practices invest in tools or staffing changes yet see little improvement in refill-related call volume. The reason is usually not technology failure, but workflow design gaps. The following mistakes commonly block meaningful reduction efforts.
- Allowing Multiple Intake Channels to Continue Unchecked: Letting patients request refills in too many ways keeps calls high and creates confusion.
- Not Requiring Complete Information Upfront: Taking refill requests without full details leads to follow-up calls and delays.
- Converting Cases Instead of Standardizing Intake: Turning calls into EHR cases doesn’t help if the intake process itself is messy.
- Automating Without Defining Exception Rules: Automation without clear rules for controlled or complex cases can create safety and compliance risks.
Best Practices to Sustain a 50% Reduction in Refill Calls
Reducing refill call volume is only half the challenge. Maintaining that reduction requires continuous monitoring, data hygiene, and workflow discipline. The practices below help prevent regression and protect long-term efficiency gains:
- Regularly Audit Flagged Refill Cases: Review exceptions and edge cases to ensure automation rules are working properly.
- Update Medication Lists Frequently: Clean, accurate medication records prevent errors and unnecessary follow-up calls.
- Communicate Refill Processes Clearly to Patients: Tell patients exactly how to request refills and what information is required, so they don’t default back to calling.
- Maintain Standard Intake Logic: Keep one clear, consistent refill process across phone, SMS, and portal. Do not let staff improvise.
- Track Metrics: Lastly, track calling metrics to identify gaps.
Here are the key refill performance metrics and why tracking them is crucial:
| Metric | Why Track It |
| Monthly refill request volume | Measure impact of workflow changes |
| Callback rate | Indicates intake completeness |
| Average time per refill case | Tracks efficiency improvements |
| Exception rate | Shows intake accuracy |
| After-hours backlog volume | Identifies staffing pressure points |
FAQs
Most refill calls happen because there is no clear, standardized process. Patients are unsure how to request refills, pharmacies send faxes, and staff often have to collect missing details, which creates repeat calls and back-and-forth.
Yes, if it replaces manual intake with a structured process. When patients are guided to submit complete refill information upfront, and routine requests are routed correctly, call volume can drop significantly.
Automation is safe for routine, same-dose refills. However, controlled substances, complex medication changes, or flagged patients should always require clinical review.
At minimum: patient name, date of birth, medication name, dosage, pharmacy, and confirmation that the medication is unchanged. Collecting complete details upfront prevents follow-up calls.
Most practices can implement standardized intake workflows within a few weeks, depending on EHR setup and staff training.
Usually the opposite. When refill requests are processed faster, and patients don’t need to wait on hold, satisfaction improves.
Trying to automate without first standardizing the intake process. If the workflow is unclear, automation alone won’t fix high call volume.
Conclusion
Prescription refill calls rarely overwhelm a practice due to excessive patient demand. The primary cause is intake friction. When requests arrive incomplete, unclear, or inconsistent, each refill requires extra steps, follow-ups, and delays.
A refill call volume drop of up to 50% starts with fixing how requests enter the workflow. With structured, validated, and standardized intake, staff no longer decode voicemails, chase missing details, or re-enter information. Nurses focus on clinical review instead of administrative rework.
Practices using Emitrr’s automated prescription refill workflows often see fewer callbacks, faster turnaround times, and a measurable drop in refill-related interruptions. Schedule a demo with Emitrr AI today to see how it works for your practice.