
Introduction
A scheduler. A nurse. An accountant. An administrative assistant.
We traced 15 healthcare CEOs back to where they started. The spotlight often falls on where leaders end up, not where they begin.
The findings surprised us, challenged a few assumptions, and left us inspired.
Meet the 15 Women Who Built Their Way Up
Every career path we studied was unique in some way. We analyzed the journeys of 15 women currently leading fast-growing healthcare organizations, but with teams of up to 200 employees. We didn’t want to look at organizations that are too big to relate to or too small to see patterns amongst.
We looked at where they started, the decisions that shaped their careers, and the common threads across their journeys.
Let’s get to know the 15 trailblazing women in healthcare who built their way to the top and became CEOs.















7 Things the Data Tells Us About Getting to the Top Job
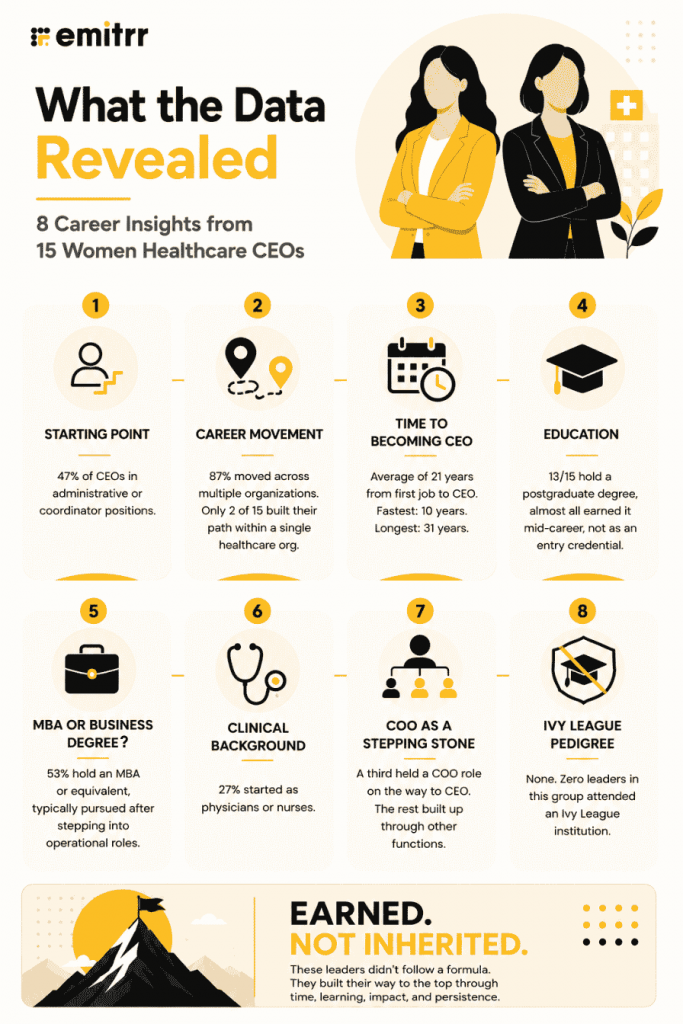
Nobody started with a clear shot at the top. Every single one of these 15 women started in a role you’d never flag as “executive material” on paper. Schedulers, bedside nurses, junior accountants, administrative assistants, and evaluation managers. Nearly half (47%) started in administrative or coordinator roles specifically, not because it was a pipeline, but because it put them closest to how a practice actually runs. The billing, the patient flow, the daily frictions nobody else wanted to own. That ground-level fluency became a competitive advantage nobody saw coming.
87% crossed multiple organizations to get there. Only 2 of 15 built their path within a single organization. The other 13 moved deliberately, picking up new functions and new scales of responsibility at each stop. Compare that to a broader healthcare CEO dataset we recently looked at (a list with predominantly men), where 60% were internal promotions.
The numbers leave us with one question.
Do men have much higher chances of being given the top job at their current employer, while women have to leave to find it?
Perhaps it’s time to rethink what the path to leadership looks like and some barriers on the way.
It took about 21 years on average. The range runs from 10 to 31 years. Kristy Needham went from collections clerk to CEO in under 20 years. Theresa Sullivan took 31, starting as an administrative assistant and accumulating functions across three decades. Karen Harwell crossed three industries entirely before landing in healthcare leadership. Tara Overmiller spent her first decade in marketing before pivoting into hospital strategy and eventually the CEO seat.
An advanced degree helps, but it follows the work, not the other way around. 87% hold a postgraduate degree, and 53% have an MBA. But almost none of them earned it before entering healthcare. Amanda Kotler was already VP of Nursing before completing her MBA. Theresa Sullivan was COO before finishing hers. The credential formalized what they were already doing operationally.

Clinical background isn’t a requirement, but it’s not enough on its own either. Four of the 15 came from clinical backgrounds. Every one of them added formal business or management training before stepping into the CEO seat. Clinical credibility opened the door. It didn’t walk them through it.
The path to CEO doesn’t always run through the COO’s office. A third held a COO role before becoming CEO. The other two-thirds got there through functional accumulation across finance, nursing, practice administration, and community relations, building enough organizational breadth that the top job became a logical next step.
These women reached the top without the signals typically associated with fast-track leadership. No Ivy League. No founder equity. No single prestigious credential. Just years of operational depth, built across multiple organizations and functions.
If leadership can take this many different paths, why do we still expect future CEOs to fit the same mold?
Conclusion
There’s no single formula here. No degree that guarantees it, no industry you have to start in, no fixed number of years you need to put in. What these 15 women share isn’t a shortcut. It’s a pattern of showing up, taking on more, and staying long enough in the work to earn the trust that comes with leading it.
For healthcare organizations, that’s worth sitting with. Your next CEO may not be on your succession plan today. She could be managing your billing team, coordinating patient schedules, leading a clinical unit, or solving operational challenges behind the scenes. The question is whether you’ll recognize that leadership potential before someone else does.
And for the women reading this, your first job doesn’t define your future. None of these leaders started with a title that hinted at the CEO’s office. They got there by growing their expertise, embracing new challenges, and continuing to move forward, one role at a time.
 4.9 (400+
reviews)
4.9 (400+
reviews)