Introduction
Over 60% of US adults manage at least one chronic condition, and chronic diseases, diabetes, hypertension, COPD, and heart disease account for the majority of healthcare spending and avoidable hospitalizations. Managing these conditions well requires far more contact than a once- or twice-a-year office visit can provide: medication adherence checks, vitals monitoring, care plan follow-up, and someone noticing early when a patient’s numbers start drifting in the wrong direction.
Patient engagement tools for chronic care span a wider range than most buyers expect, from dedicated CCM/RPM billing platforms to enterprise population-health analytics engines that power care management at ACO scale, to specialized data and consulting partners that plug into a broader chronic care strategy. This guide evaluates 10 platforms across that full range, covering CMS-reimbursed care management software, analytics-driven risk stratification platforms, and the specialized SDOH and integration partners that often sit underneath a mature chronic care program.

How We Evaluated These Apps
To build this guide, we evaluated each platform against the dimensions that matter most for chronic care, specifically: CMS compliance infrastructure (accurate time tracking, audit-ready documentation, billing automation for CCM/RPM/BHI/TCM codes where applicable), risk stratification and predictive analytics depth, patient engagement and adherence tools, EHR/claims integration depth, care coordination workflow support, and pricing transparency.
We treat “chronic care” tools as a category spanning genuinely different operational layers, not a single comparable feature set. Some platforms here are CMS-billing-focused CCM/RPM engines built for individual practices; others are enterprise analytics and network-performance platforms that ACOs and health systems use to power chronic disease risk stratification and care management at scale; and others are specialized partners, SDOH data, custom integration, outsourced panel management, that plug into a broader chronic care strategy rather than running it end-to-end. We evaluate each on what it’s actually built to do.
Our evaluation drew on vendor documentation, G2, Capterra, KLAS Research, and independent industry comparisons, with data compiled as of June 2026. Pricing in this category is rarely fully published, especially for enterprise and revenue-share models. Always request a quote, modeling your specific patient panel.
Patient Engagement Tools for Chronic Care at a Glance (TL;DR)
| Platform | Category | Best For | EHR/Data Integration | Pricing |
| Emitrr | Engagement/automation layer | All-in-one outreach, reminders, and adherence communication | Athena, Tebra, ECW + 500 more | ~$99/month |
| HealthSnap | Device-centric RPM + CCM | Cellular RPM devices bundled tightly with CCM | EHR-integrated | Custom |
| ChronicCareIQ | Software-only, device-integrated | Diabetes/hypertension-focused CCM+RPM with CGM integration | EHR integration, custom | Custom |
| ChartSpan | Full-service, revenue-share | Practices wanting turnkey CCM with zero internal staffing | Major EHRs (Epic, Cerner) | Revenue-share |
| Welkin Health | Software-only, codeless config | Behavioral health and complex multi-condition chronic care | API + codeless integrations | Custom quote |
| Athenahealth | Enterprise EHR + chronic care module | Ambulatory practices managing chronic disease across multi-EHR locations | Native + cross-platform | Custom, practice-based |
| Arcadia | Enterprise analytics & risk stratification | ACOs/health systems needing predictive chronic disease risk stratification | Claims + clinical, EHR-agnostic | Custom enterprise |
| J2 Interactive | Custom integration/consulting | Health systems needing custom chronic care coordination builds | Project-based, any EHR | Custom project pricing |
| HealthHelper | Outsourced panel/care gap management | Practices wanting chronic disease care gap closure as a managed service | Works with any EHR | Performance-based, modular |
| Socially Determined | SDOH data & social risk intelligence | Factoring social risk into chronic disease risk stratification | API/data ingestion | Custom enterprise |
What Are Patient Engagement Tools for Chronic Care?
Patient engagement solutions for chronic care are technologies and strategies designed to actively involve patients in their own healthcare journey, particularly those managing long-term health conditions. These tools go beyond traditional communication methods, aiming to educate, motivate, and support patients in adhering to their treatment plans, making informed lifestyle choices, and collaborating effectively with their care teams.
The core idea is to empower patients by providing them with the resources, information, and support they need to manage their conditions effectively on a daily basis. This is crucial because chronic disease management isn’t just about what happens in the clinic; it’s about consistent self-care, adherence to medication, monitoring symptoms, and adopting healthy behaviors between appointments.
These tools can take many forms, including:
- Digital platforms: Mobile apps, patient portals, and web-based dashboards.
- Communication technologies: Secure messaging, automated reminders, and telehealth services.
- Remote monitoring devices: Wearable sensors and connected home health devices.
- Educational resources: Interactive content, personalized health plans, and video libraries.
The goal is to create a continuous feedback loop between patients and providers, ensuring that care is personalized, timely, and effective.
Why Patient Engagement Tools Are Essential for Chronic Care
Patient engagement tools play a critical role in chronic disease management by keeping patients connected to their care teams between office visits. They improve medication adherence, automate proactive outreach, support care coordination, and enable providers to monitor patient progress continuously. As healthcare shifts toward value-based care, these tools have become essential for improving outcomes, reducing costs, and delivering personalized care at scale.
Improve Clinical Outcomes
Engaged patients are more likely to actively participate in managing their health, resulting in better long-term outcomes. Patient engagement tools help providers:
- Improve chronic disease management through medication reminders, education, and regular follow-ups.
- Increase medication adherence and encourage healthier lifestyle changes.
- Reduce preventable complications associated with conditions such as diabetes, hypertension, COPD, and heart disease.
- Increase preventive care participation, including screenings, vaccinations, and annual wellness visits.
- Lower hospitalizations, emergency department (ED) visits, and avoidable readmissions through proactive intervention.
Enhance Patient Experience
Modern patient engagement platforms make healthcare more accessible, personalized, and convenient throughout the patient journey.
Key benefits include:
- Personalized communication based on patient conditions and care plans.
- Convenient access through SMS, voice calls, patient portals, and telehealth.
- Two-way communication that allows patients to ask questions, schedule appointments, and stay connected with care teams.
- Greater patient satisfaction by empowering individuals to take an active role in their healthcare.
Reduce Healthcare Costs and Improve Operational Efficiency
Chronic diseases account for a significant portion of healthcare utilization and spending. Patient engagement tools reduce costs by replacing manual outreach with automated workflows and focusing resources on patients who need intervention the most.
Healthcare organizations benefit from:
- Fewer emergency department visits and hospital readmissions.
- Automated care gap detection, automated appointment reminders, and follow-up workflows.
- Predictive analytics and risk stratification that prioritize outreach for high-risk patients.
- Better resource allocation by reducing manual chart reviews and repetitive administrative work.
- Automated documentation and time tracking that support Chronic Care Management (CCM) and Remote Patient Monitoring (RPM) billing requirements.
Support Value-Based Care and Population Health
Patient engagement is a core component of population health management and value-based care (VBC) programs. By improving patient participation and closing care gaps, healthcare organizations can achieve better quality outcomes while reducing overall costs.
Patient engagement tools help organizations:
- Improve HEDIS, Star Ratings, and other quality performance measures.
- Support Accountable Care Organizations (ACOs) and shared savings initiatives.
- Identify high-risk patients using AI-powered risk stratification and predictive analytics.
- Incorporate Social Determinants of Health (SDOH) into care planning for more equitable healthcare delivery.
- Improve financial performance under value-based reimbursement models.
Why Traditional Chronic Care Programs Fall Short
Managing chronic disease through manual processes is no longer sustainable. Providers often struggle to identify high-risk patients, perform consistent outreach, and maintain continuous engagement across large patient populations.
Modern patient engagement tools address these challenges by providing:
- Automated risk stratification and care gap identification.
- AI-powered, targeted patient outreach instead of one-size-fits-all communication.
- Continuous patient engagement beyond scheduled office visits.
- Integrated care coordination, automated workflows, and compliance support.
- 24/7 communication channels that help organizations meet CMS Chronic Care Management (CCM) requirements while improving patient access to care.
What to Look for in Patient Engagement Tools for Chronic Care
Choosing the right patient engagement platform goes beyond messaging capabilities. The best solutions combine care coordination, automation, analytics, compliance, and EHR integration to support long-term chronic disease management while improving clinical and financial outcomes.
Compliance and Billing Support
If your organization participates in Chronic Care Management (CCM), Remote Patient Monitoring (RPM), or other reimbursement programs, the platform should simplify compliance and documentation.
Look for features such as:
- Automatic time tracking and audit-ready documentation for CCM and RPM billing.
- Support for multiple billing programs, including CCM, Complex CCM, RPM, Behavioral Health Integration (BHI), and Transitional Care Management (TCM).
- Social Determinants of Health (SDOH) screening and documentation to meet evolving CMS requirements.
Risk Stratification and Population Health Analytics
Strong patient engagement platforms help providers identify which patients need intervention before complications occur.
Key capabilities include:
- Dynamic risk stratification using clinical, claims, utilization, and SDOH data.
- Predictive analytics to identify patients at risk for hospitalization, readmission, or disease progression.
- Real-time cohort updates that automatically refresh patient risk scores and outreach lists.
- Demonstrated outcomes, such as reduced emergency department visits, hospital readmissions, or improved chronic disease management.
Patient Engagement and Communication
Effective patient engagement depends on consistent, personalized communication across multiple channels.
Look for platforms that offer:
- Two-way texts, voice, email, mobile apps, or patient portals.
- Automated outreach for missed appointments, medication adherence, preventive care, and follow-up reminders.
- Proactive non-adherence alerts that trigger outreach when patients miss monitoring activities or scheduled care.
- Multilingual communication to improve engagement across diverse patient populations.
Integration and Care Coordination
These tools should integrate seamlessly with existing healthcare systems and support collaboration across care teams.
Important capabilities include:
- Two-way EHR and claims integration to synchronize patient records, care gaps, and outreach activities.
- Care coordination workflows that support task assignment, referrals, team collaboration, and patient handoffs.
- Shared visibility into patient communication and care plans across multidisciplinary teams.
Scalability and Operational Fit
The right platform should align with your organization’s size, care model, and operational resources.
When evaluating vendors, consider:
- Whether the platform offers a software-only solution, managed services, analytics, or a full-service chronic care management program.
- Scalability for independent practices, multispecialty groups, health systems, ACOs, and value-based care organizations.
- Remote Patient Monitoring (RPM) support, including device logistics, patient onboarding, shipping, and equipment management, where applicable.
Looking to improve chronic care workflows with AI? Watch this video to discover the top 5 AI tools transforming patient engagement and care management.
Top 10 Patient Engagement Tools for Chronic Care: In-Depth Comparison
- Emitrr
- HealthSnap
- ChronicCareIQ
- ChartSpan
- Welkin Health
- Athenahealth
- Arcadia
- J2 Interactive
- HealthHelper
- Socially Determined
1. Emitrr (Best for All-in-One Outreach and Adherence Communication)
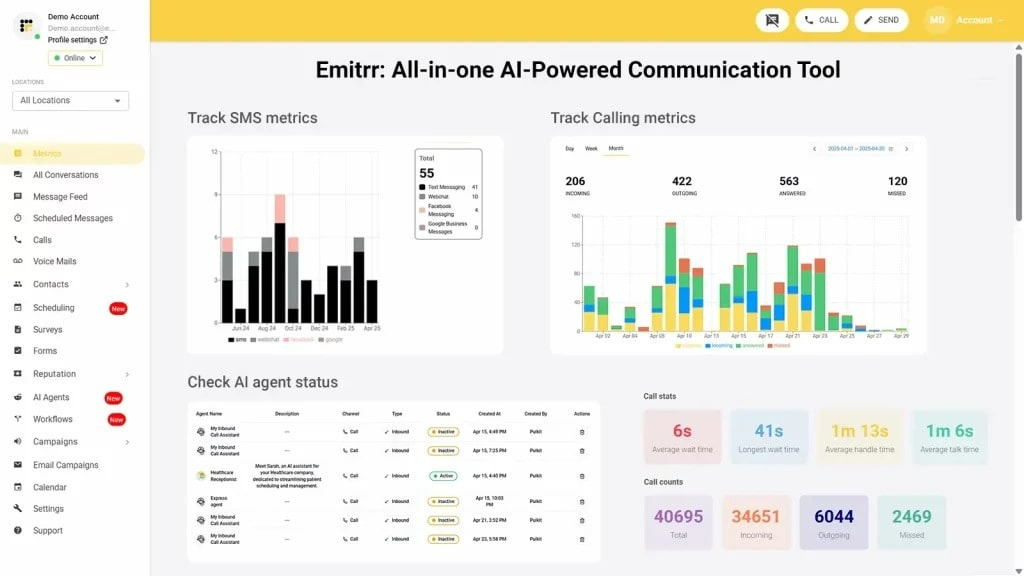
Ideal For: Practices wanting a flexible patient engagement platform that combines AI voice, SMS outreach, care coordination, and adherence automation while working alongside existing CCM, RPM, or population health programs.
Emitrr Overview
Emitrr helps healthcare organizations improve chronic care engagement through automated patient communication, AI-powered voice and SMS agents, and workflow automation. Rather than replacing CCM or RPM platforms, it strengthens patient adherence and follow-up by keeping outreach consistent, personalized, and connected to EHR workflows.
Emitrr Key Features
- Two-way text and AI voice outreach for reminders, patient recalls, chronic care management, and preventive care campaigns.
- Dynamic patient segmentation using EHR data, diagnoses, demographics, and appointment history.
- Visual workflow builder with triggers, conditional logic, automated text messaging, forms, and task creation.
- AI voice and SMS agents that automate patient conversations while escalating complex requests to staff.
- Native EHR integrations with Athenahealth and eClinicalWorks for closed-loop workflows.
Emitrr Pros
- Combines patient outreach, AI automation, communication, and care coordination in one platform.
- HIPAA-compliant texting with BAAs, secure communication, and consent management included.
- Shared SMS inbox and automated routing improve multidisciplinary care coordination.
- Flexible deployment with phased implementation options.
- Supports multilingual communication through SMS, voice, and web chat.
- Transparent pricing compared to enterprise-only alternatives.
Emitrr Cons
- Healthcare businesses pay an additional setup fee to unlock advanced automation
- AI capabilities require upgrading to the Pro plan
- Multi-party group chat threading is still evolving
- Enterprise pricing requires contacting sales
When NOT to Choose Emitrr
Choose another solution if you need a complete CCM billing platform or enterprise population health analytics with built-in claims management.
Emitrr Pricing
Starts at approximately $99/month, with custom pricing available based on patient volume and automation requirements.
- MailChimp
- Denticon
- AthenaHealth
- Zapier
- Salesforce
- HouseCall Pro
- + 500 more!!
Emitrr Rating
Capterra: 4.6/5 (June 2026)
Emitrr Support Channels
- Email Support
- Phone Support
- Live Chat
- Knowledge Base
- Customer Success Team
2. HealthSnap (Best for Cellular-Based RPM Bundled with CCM)
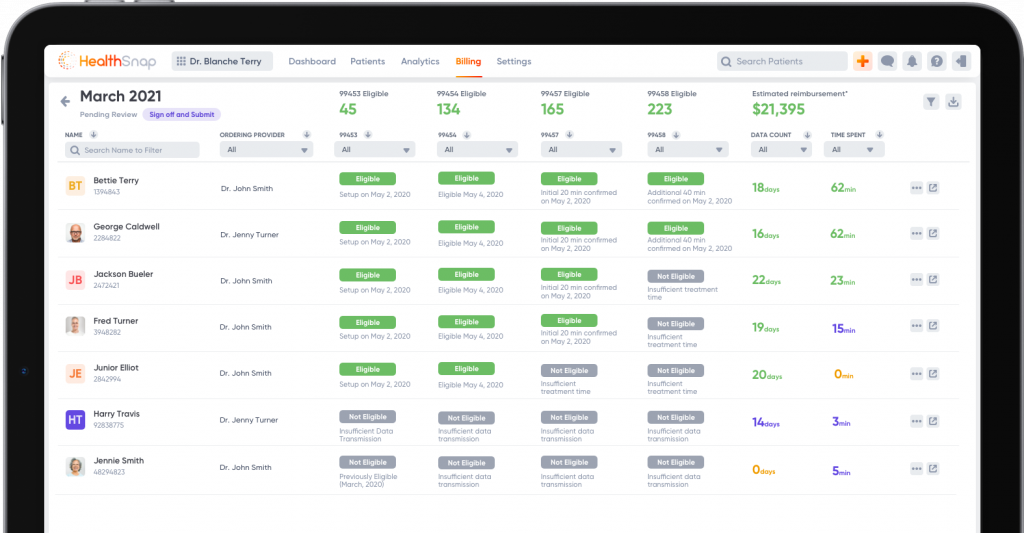
Ideal For: Healthcare providers looking to combine Chronic Care Management and Remote Patient Monitoring using cellular-connected medical devices with minimal patient setup.
HealthSnap Overview
HealthSnap is a chronic disease management platform that combines CCM and RPM into a single solution. Its cellular-enabled monitoring devices eliminate the need for Wi-Fi or smartphones while giving care teams real-time patient data and supporting Medicare reimbursement programs.
HealthSnap Key Features
- Cellular-connected RPM devices requiring no smartphone pairing.
- Real-time dashboards for monitoring chronic disease trends.
- Combined CCM and RPM reimbursement support.
- HIPAA-compliant device management and monitoring.
HealthSnap Pros
- Excellent solution for practices running combined CCM and RPM programs.
- Cellular connectivity improves patient compliance.
- Supports proactive interventions through real-time monitoring.
- Purpose-built for chronic disease management.
HealthSnap Cons
- Focuses primarily on RPM-centered care programs.
- Requires device deployment and ongoing hardware management.
- Smaller market presence than some established competitors.
When NOT to Choose HealthSnap
Skip HealthSnap if your chronic care program does not include remote patient monitoring devices.
HealthSnap Pricing
Custom pricing based on program size, devices, and implementation requirements.
HealthSnap Integrations
- EHR Systems
- Billing Platforms
- RPM Device Integrations
HealthSnap Rating
No reviews available
HealthSnap Support Channels
- Email Support
- Customer Success Team
- Training Resources
- Technical Support
3. ChronicCareIQ (Best for Diabetes and Hypertension-Focused CCM + CGM Integration)
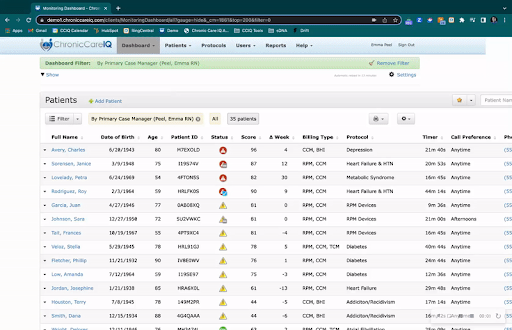
Ideal For: Practices specializing in diabetes and hypertension management that need AI-powered continuous glucose monitoring, automated coaching, and streamlined chronic care workflows.
ChronicCareIQ Overview
ChronicCareIQ combines continuous glucose monitoring with AI-powered patient coaching and predictive analytics. The platform is designed to improve chronic disease management while supporting Medicare billing for RPM and CCM programs.
ChronicCareIQ Key Features
- Continuous glucose monitoring integration.
- Automated patient coaching through a mobile application.
- Predictive analytics for diabetes and hypertension management.
- Automated billing support for RPM and CCM services.
- Connected device integrations.
ChronicCareIQ Pros
- Strong specialization in diabetes management.
- AI-driven predictive insights improve patient outcomes.
- High patient engagement through personalized coaching.
- Simplifies billing and EHR documentation.
ChronicCareIQ Cons
- Primarily focused on diabetes and hypertension.
- Requires connected medical devices and onboarding.
When NOT to Choose ChronicCareIQ
Choose another platform if your chronic care program includes a broad range of chronic diseases beyond diabetes and hypertension.
ChronicCareIQ Pricing
Custom pricing based on organization size and monitoring requirements.
ChronicCareIQ Integrations
- EHR Systems
- Continuous Glucose Monitoring Devices
- Connected Medical Devices
ChronicCareIQ Rating
Limited publicly available ratings across major review platforms.
ChronicCareIQ Support Channels
- Email Support
- Technical Support
- Customer Success Team
- Training Resources
4. ChartSpan (Best Turnkey Full-Service CCM Program)
Ideal For: Primary care and internal medicine practices looking to outsource chronic care management while generating CCM reimbursement without hiring additional care coordinators.
ChartSpan Overview
ChartSpan provides a fully managed chronic care management program where dedicated clinical staff handle patient enrollment, monthly outreach, documentation, and compliance while practices receive Medicare reimbursement through a revenue-sharing model.
ChartSpan Key Features
- Managed patient enrollment and monthly outreach.
- Clinical documentation and CCM compliance tracking.
- Revenue-share billing model.
- Remote Patient Monitoring support.
- Major EHR integrations.
ChartSpan Pros
- Minimal operational burden for practices.
- Well-established national CCM provider.
- No upfront software investment.
- Supports both CCM and RPM programs.
ChartSpan Cons
- Revenue-sharing reduces overall reimbursement.
- Limited workflow customization.
- Patient communication depends on outsourced care teams.
When NOT to Choose ChartSpan
Avoid ChartSpan if you already have an internal care management team and prefer to keep full reimbursement revenue.
ChartSpan Pricing
ChartSpan provides custom pricing based on practice type and Medicare reimbursement rates. Patient costs depend on insurance and applicable copays or deductibles.
ChartSpan Integrations
- Epic
- Cerner
- Major EHR Systems
ChartSpan Rating
Limited publicly available ratings across major review platforms.
ChartSpan Support Channels
- Dedicated Care Team
- Technical Support
- Customer Success
- Training Resources
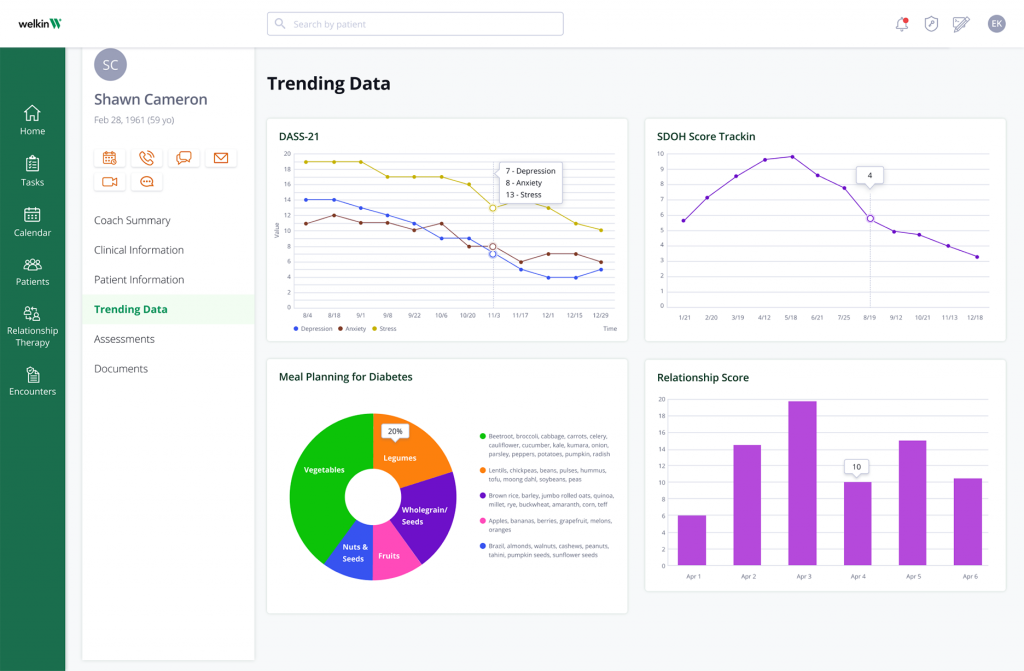
5. Welkin Health (Best for Behavioral Health and Complex Multi-Condition Chronic Care)
Ideal For: Healthcare organizations managing behavioral health and complex chronic disease populations that require highly customizable care plans and collaborative care coordination.
Welkin Health Overview
Welkin Health is a care management platform that enables organizations to design flexible chronic care workflows using codeless tools. It supports multidisciplinary care teams with secure communication, analytics, and customizable care plans for complex patient populations.
Welkin Health Key Features
- Codeless care plan builder.
- Multi-channel patient communication including secure video, SMS, MMS, and email.
- Integration with over 110 laboratory providers.
- Embedded analytics for chronic care programs.
Welkin Health Pros
- Excellent flexibility for behavioral health and complex chronic care.
- Strong communication capabilities across multiple channels.
- HIPAA compliant and SOC 2 Type II certified.
- Supports highly customized care management workflows.
Welkin Health Cons
- Not specifically designed as a CCM billing platform.
- Enterprise pricing requires contacting sales.
- Limited publicly available customer reviews.
When NOT to Choose Welkin Health
Choose another solution if your primary objective is maximizing Medicare CCM or RPM reimbursement rather than building highly customized care programs.
Welkin Health Pricing
Custom enterprise pricing available upon request.
Welkin Health Integrations
- APIs
- Rcopia e-Prescribing
- 110+ Laboratory Vendors
- Healthcare Data Connectors
Welkin Health Rating
No major third-party rating available, though healthcare organizations consistently praise its flexibility and communication capabilities.
Welkin Health Support Channels
- Email Support
- Customer Success
- Implementation Team
- Technical Support
- Knowledge Base
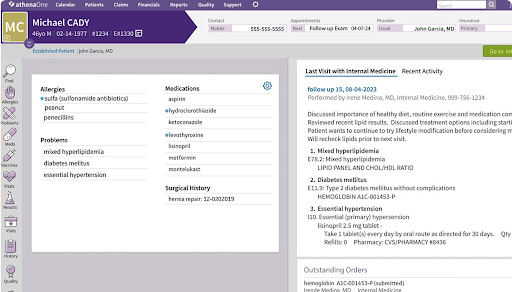
6. Athenahealth (Best Multi-EHR Chronic Care Management for Ambulatory Practices)
Ideal For: Primary care practices, specialty clinics, and FQHCs managing chronic disease populations across multiple locations and multiple EHR systems.
Athenahealth Overview
Athenahealth combines chronic care management capabilities with its EHR and practice management platform, enabling practices to manage chronic disease populations through automated outreach, predictive analytics, and patient engagement. Its cross-platform interoperability makes it especially useful for organizations operating across multiple locations or different EHR environments.
Athenahealth Key Features
- Chronic care management modules integrated into the Athenahealth practice management platform.
- Automated patient outreach for chronic disease follow-ups and care gap closure.
- Predictive risk scoring to identify high-risk patients requiring proactive intervention.
- Patient engagement portal and mobile app for care plans, messaging, and appointment management.
Athenahealth Pros
- Ideal for practices already using Athenahealth as their EHR and practice management system.
- Supports cross-EHR interoperability for organizations managing multiple locations.
- Patient portal integration encourages ongoing engagement and self-service.
- Combines clinical, administrative, and engagement tools within a single ecosystem.
Athenahealth Cons
- Delivers the most value when Athenahealth is the organization’s primary EHR.
- Risk stratification capabilities are less advanced than dedicated analytics platforms.
- Chronic care pricing is not publicly available.
When NOT to Choose Athenahealth
Choose another solution if you don’t use Athenahealth as your core practice management platform or need enterprise-level chronic disease analytics and predictive modeling.
Athenahealth Pricing
Custom pricing based on practice size and selected modules.
Athenahealth Integrations
- Athenahealth EHR
- Cross-platform EHR interoperability
- Patient Portal
- Practice Management Suite
Athenahealth Rating
Gartner: 4/5
Athenahealth Support Channels
- Phone Support
- Email Support
- Customer Portal
- Knowledge Base
- Training Resources
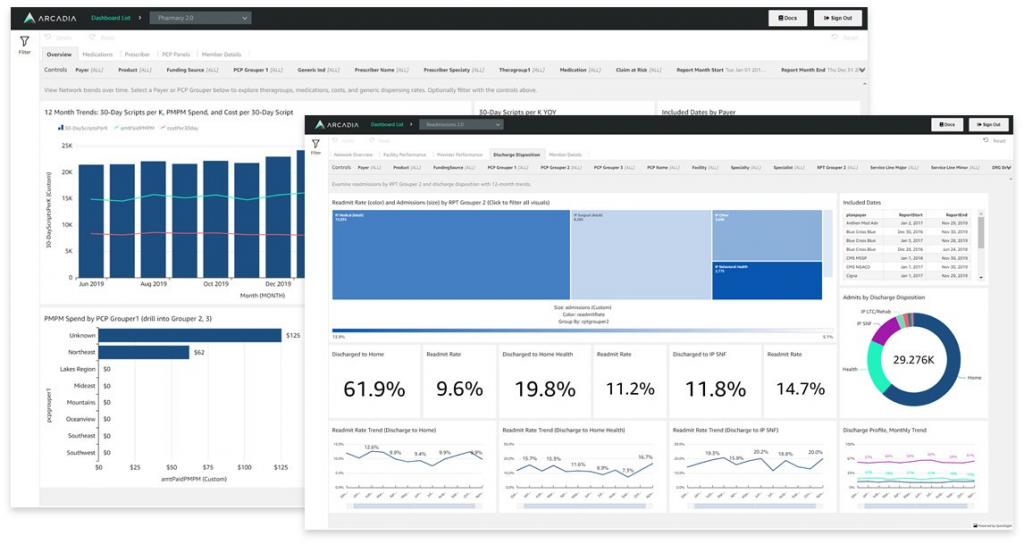
7. Arcadia (Best for Enterprise Chronic Disease Risk Stratification)
Ideal For: ACOs, health systems, and provider networks that require enterprise-scale predictive analytics and chronic disease risk stratification.
Arcadia Overview
Arcadia is an enterprise healthcare analytics platform that combines clinical, claims, and social determinants of health data to identify high-risk chronic disease patients and prioritize care management. Its predictive analytics help organizations intervene earlier and improve outcomes across large patient populations.
Arcadia Key Features
- Patient registry with clinical, demographic, utilization, and cost-based risk profiling.
- Predictive analytics for hospitalization and disease progression risk.
- Dynamic patient cohorts updated continuously using real-time claims and clinical data.
- Support for CMS value-based care initiatives and specialty care models.
Arcadia Pros
- Proven improvements in chronic disease outcomes and emergency department utilization.
- Supports significantly larger patient populations without increasing care management staff.
- Industry-leading predictive analytics and risk stratification capabilities.
- Highly regarded by KLAS and Black Book for population health analytics.
Arcadia Cons
- Complex implementation for organizations with fragmented data environments.
- Patient engagement requires integration with separate communication platforms.
- Enterprise pricing only with no publicly available plans.
- Better suited for large provider organizations than independent practices.
When NOT to Choose Arcadia
Avoid Arcadia if you need built-in patient communication tools or operate a small practice without enterprise-level analytics requirements.
Arcadia Pricing
Custom enterprise pricing.
Arcadia Integrations
- EHR-Agnostic Data Integration
- Claims Data Feeds
- AWS-Based Data Platform
- Clinical and SDOH Data Sources
Arcadia Rating
No major third-party rating available, though healthcare organizations consistently praise its flexibility and communication capabilities.
Arcadia Support Channels
- Enterprise Support
- Customer Success Team
- Technical Support
- Documentation
- Implementation Services
8. J2 Interactive (Best for Custom Chronic Care Coordination Builds)
Ideal For: Health systems and provider organizations requiring custom-built chronic care coordination and patient engagement solutions.
J2 Interactive Overview
J2 Interactive is a healthcare IT consulting and software development firm specializing in custom chronic care coordination, interoperability, and CRM-based patient engagement solutions. Rather than offering an off-the-shelf platform, it builds solutions tailored to complex healthcare workflows.
J2 Interactive Key Features
- Custom chronic care coordination and patient journey development.
- Salesforce healthcare CRM implementations.
- Post-discharge care coordination solutions.
- Advanced EHR integration with InterSystems technologies.
J2 Interactive Pros
- Multiple Best in KLAS awards for Technical Services.
- Over two decades of healthcare integration experience.
- Flexible enough to support highly customized chronic care workflows.
- Strong employee satisfaction reflecting delivery quality.
J2 Interactive Cons
- Consulting engagement rather than ready-to-use software.
- Pricing depends entirely on project scope.
- Longer implementation timelines than SaaS platforms.
- Best suited for organizations with dedicated implementation resources.
When NOT to Choose J2 Interactive
Choose another platform if you need an out-of-the-box chronic care management solution that can be deployed quickly.
J2 Interactive Pricing
Custom project-based pricing.
J2 Interactive Integrations
- InterSystems IRIS
- InterSystems HealthShare
- Salesforce Healthcare CRM
- Custom EHR Integrations
J2 Interactive Rating
No reviews are available
J2 Interactive Support Channels
- Dedicated Project Team
- Technical Support
- Consulting Services
- Training
- Documentation
9. HealthHelper (Best Outsourced Chronic Disease Care Gap Closure Service)
Ideal For: Primary care practices seeking outsourced chronic disease outreach and care coordination without hiring an internal care management team.
HealthHelper Overview
HealthHelper combines technology with dedicated care coordinators who work directly within a practice’s EHR to identify patients needing outreach, close care gaps, and improve chronic disease outcomes while reducing staff workload.
HealthHelper Key Features
- Chronic disease panel analytics for identifying patients requiring outreach.
- Care Gap Helper for diabetes, hypertension, screenings, and preventive care.
- Multi-channel scheduling via SMS, patient portal, email, and phone.
- Coordinators documenting directly within the practice’s EHR.
HealthHelper Pros
- Demonstrated improvements in HEDIS performance and patient engagement.
- Proven ROI through documented case studies.
- Compatible with virtually any EHR.
- Fast implementation with most deployments completed in 4–6 weeks.
HealthHelper Cons
- Combines software with outsourced staffing rather than being self-service.
- Pricing varies by engagement and isn’t publicly available.
- Primarily designed for primary care organizations.
- Limited independent review coverage.
When NOT to Choose HealthHelper
Avoid HealthHelper if you want full control over outreach workflows using an internally managed software platform.
HealthHelper Pricing
Performance-based custom pricing.
HealthHelper Integrations
- Compatible with Any EHR
- Practice Management Systems
HealthHelper Rating
No reviews are available
HealthHelper Support Channels
- Dedicated Care Coordinators
- Customer Success Team
- Technical Support
- Implementation Services
10. Socially Determined (Best for SDOH Data in Chronic Disease Risk Stratification)

Ideal For: Healthcare organizations requiring person-level social determinants of health data to improve chronic disease risk assessment and intervention planning.
Socially Determined Overview
Socially Determined’s SocialScape platform delivers highly granular social risk intelligence, helping providers identify non-clinical factors such as housing, transportation, food insecurity, and financial challenges that directly affect chronic disease outcomes and medication adherence.
Socially Determined Key Features
- Person-level social risk scoring across multiple SDOH domains.
- Geospatial analytics with resolution down to approximately 200 meters.
- Claims data matching for comprehensive health and social risk profiles.
- HITRUST-certified data platform.
Socially Determined Pros
- One of the most detailed SDOH datasets available.
- Helps identify barriers to chronic disease adherence beyond clinical factors.
- Strong customer feedback regarding actionable insights.
- Backed by healthcare-focused investors and significant funding.
Socially Determined Cons
- Provides data intelligence rather than patient engagement or care coordination.
- Enterprise pricing only.
- Best used alongside broader chronic care platforms.
- Does not include outreach automation or workflow management.
When NOT to Choose Socially Determined
Choose another platform if you need a complete chronic care management solution with built-in communication and patient outreach.
Socially Determined Pricing
Custom enterprise pricing.
Socially Determined Integrations
- API-Based Data Integration
- Claims Data Integration
- Population Health Platforms
- Care Management Systems
Socially Determined Rating (Source)
No reviews are available
Socially Determined Support Channels
- Enterprise Support
- Customer Success
- Advisory Services
- Technical Support
- Documentation
Which Patient Engagement Tool for Chronic Care Is Right for You?
| Your Situation | Best Choice | Why |
| Want an all-in-one outreach/automation layer underneath any model | Emitrr | Flexible AI voice/SMS engagement, accessible pricing |
| Want cellular RPM devices bundled tightly with CCM | HealthSnap | Cellular-connected devices, real-time insights, CCM+RPM bundling |
| Diabetes/hypertension-focused panel wanting CGM integration | ChronicCareIQ | AI-driven predictive insights tuned specifically to CGM data |
| Want a fully turnkey CCM program with zero internal staffing | ChartSpan | Largest, most established full-service revenue-share model |
| Running behavioral health or complex multi-condition programs | Welkin Health | Codeless care plan design, strong multi-channel communication |
| Ambulatory practice already using Athenahealth as core EHR/PM | Athenahealth | Cross-platform chronic care management built into the existing ecosystem |
| ACO/health system needing enterprise chronic disease risk stratification | Arcadia | Documented 41.5% ED visit reduction for COPD, 3x patient capacity |
| Need a custom-built solution for unusual chronic care workflows | J2 Interactive | Best in KLAS Technical Services, deep EHR integration expertise |
| Want chronic disease care gap closure without building an outreach team | HealthHelper | Tech-enabled service, documented 31% HEDIS improvement |
| Need granular SDOH data for chronic disease risk stratification | Socially Determined | Person-level social risk scoring at 200-meter resolution |
Key Takeaways
- Chronic care engagement tools span very different organizational layers: individual-practice billing/engagement tools (Emitrr, HealthSnap, ChronicCareIQ, ChartSpan, Welkin Health), ambulatory EHR-embedded chronic care (Athenahealth), enterprise risk stratification (Arcadia), and specialized partners (J2 Interactive, HealthHelper, Socially Determined) — match the platform to your organizational scale, not just the “chronic care” label.
- The 2026 Medicare Physician Fee Schedule increased CCM/RPM reimbursement and added new flexible billing codes, while CMS’s incoming Ambulatory Specialty Model places direct financial weight on heart failure and low back pain risk stratification starting in 2027.
- Predictive, risk-based outreach prioritization consistently outperforms uniform outreach — documented results include a 41.5% reduction in ED visits for COPD patients and a 31% improvement in HEDIS measures from real deployments.
- Social determinants of health materially affect chronic disease management success, particularly medication adherence, programs that ignore SDOH data in risk stratification will underperform in underserved populations.
- Two-way EHR integration, writing outreach activity and care gap status back, not just reading data, is the biggest differentiator between platforms that genuinely close the loop and those that just generate reports.
- Automatic time tracking and audit-ready documentation remain non-negotiable for any platform involved in CCM/RPM billing, regardless of how sophisticated its engagement or analytics layer is.
Frequently Asked Questions
Reputable platforms in this category should be HIPAA compliant with a signed BAA, encrypted data handling, and SOC 2 certification where applicable. Always confirm current compliance documentation directly with any vendor before deployment.
SDOH data — housing stability, food security, transportation access — helps identify the actual barrier behind chronic disease non-adherence. A patient who isn't picking up refills due to transportation issues needs a different intervention than one who's simply forgetting; SDOH-informed risk stratification surfaces that distinction, which clinical data alone misses.
Small practices typically do best with a full-service vendor (ChartSpan) to avoid internal staffing burden, a device-bundled option (HealthSnap, ChronicCareIQ) if RPM is central to the program, or an accessible engagement-layer tool like Emitrr if some internal capacity already exists.
Arcadia is purpose-built for enterprise-scale chronic disease risk stratification with documented outcomes, while Athenahealth serves ambulatory networks already on its EHR, and J2 Interactive is the right fit when chronic care coordination needs don’t match any standard product.
The primary goal is to empower patients to actively participate in managing their long-term health conditions. This involves providing them with the necessary information, support, and motivation to adhere to treatment plans, make healthy lifestyle choices, and collaborate effectively with their healthcare providers, ultimately leading to improved health outcomes and quality of life.
Patient engagement tools help reduce costs by preventing costly acute events such as hospitalizations and emergency room visits. By improving adherence to medication and care plans, enabling early detection of issues through remote monitoring, and promoting preventive care, these tools minimize the progression of chronic diseases and their associated complications, leading to lower overall healthcare expenditures.
Patient portals provide patients with secure access to their health records, appointment scheduling, prescription refill requests, and direct messaging with their care team. For chronic disease management, this means patients can easily track their progress, communicate concerns promptly, receive reminders for tests or medications, and access educational materials tailored to their condition, fostering better self-management and adherence.
Population health management is the overarching strategy and set of processes aimed at improving the health of a defined patient population. It involves analyzing data, stratifying risk, and coordinating care across groups. Patient engagement is a critical component within population health management; it's the set of tactics and tools used to actively involve individual patients in their own care, making the broader population health strategy effective.
Yes, RPM devices can be crucial for early detection. For example, a connected blood pressure cuff can alert a care team to dangerously high readings, or a glucose meter can signal uncontrolled blood sugar levels in a diabetic patient. This early warning allows for timely intervention, potentially preventing serious complications, hospitalizations, or emergency room visits.
Final Verdict
Effective chronic care management requires more than periodic check-ins—it demands consistent patient engagement, proactive outreach, and streamlined communication between visits. While many chronic care management platforms help with care coordination, documentation, and remote monitoring, practices also need a reliable way to keep patients connected throughout their care journey.
Emitrr complements chronic care management by combining AI-powered patient communication, automated reminders, two-way texting, voice AI, and seamless EHR integrations to help practices improve engagement, reduce administrative workload, and support better long-term patient outcomes.
Ready to enhance your chronic care management program? Schedule a personalized demo with Emitrr and see how AI-powered communication can help your team deliver more connected, efficient, and patient-centered care.
 4.9 (400+
reviews)
4.9 (400+
reviews)